Chemotherapy-Induced Nausea and Vomiting Updated
Background
Although significant improvements have been made in the management of chemotherapy-induced nausea and vomiting (CINV), this side effect continues to be one of the most distressing symptoms associated with cancer treatment.1 CINV has the potential to affect patients’ quality of life (QoL) and can lead to decreased treatment adherence for some patients.2,3 The primary goal of antiemetic therapy is to completely control or minimize the symptom of CINV.3
In the 1960’s through the late 1980’s, treatment of CINV primarily involved the use of dopamine antagonists, such as prochlorperazine and metoclopromide; the introduction of the serotonin antagonists two decades ago vastly improved the control of this symptom. However, patients continued to suffer from CINV despite the best treatments (including the serotonin antagonists) available to health care providers (HCP). In fact, the symptom of delayed nausea and vomiting became even more apparent after the introduction of serotonin antagonists, probably because the acute period was better controlled.4
The approval of a long acting serotonin antagonist (palonosetron, Aloxi®) in 2003 was a significant addition to the existing armamentarium of antiemetic agents as it extended the activity of the drug with its prolonged half-life of 40 hours. In addition, the 2003 approval of a novel new class of agent, the neurokinin 1 (NK-1) receptor antagonist (aprepitant,Emend®), was a critical advancement in the field of antiemetic therapy, offering patients a unique treatment that targeted a new receptor and was aimed at both the acute period of CINV and the more problematic delayed period following chemotherapy.
Classification of CINV
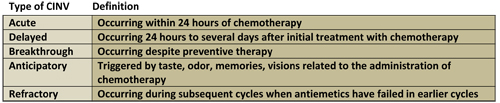
Based on information from Hawkins & Grunberg, 20095
Scope of the Problem
Antiemetic regimens, including the therapeutic standard of serotonin receptor antagonists and corticosteroids, vastly improved the control of CINV in patients receiving chemotherapy.6 Although the control of the acute period of nausea and vomiting improved and vomiting occurred less, studies indicated that the incidence of nausea may have risen despite the reduction in vomiting. In a prospective, multicenter, multinational study of 298 patients receiving highly emetogenic chemotherapy (HEC) or moderately emetogenic chemotherapy (MEC), CINV was found to adversely affect patients’ quality of life (QoL) despite antiemetic therapy; nausea was found to more distressing than vomiting.6
An oft quoted study by Grunberg et al.7 markedly illustrates the disconnect between HCP perception of CINV among patients receiving chemotherapy compared to the actual CINV experienced by the patients as recorded by diary. Adult patients receiving HEC or MEC for the first time were enrolled in a prospective, observational study; prior to enrollment, medical oncologists and oncology nurses (n=24) estimated the incidence of acute (day 1) and delayed (days 1-5) CINV following HEC or MEC chemotherapy from their own practices. The study took place in practices located in Denmark, France, Italy, Germany, the U.K., and the U.S. during 2001–2002.7 The participating patients (n=298) completed a 6 day diary reporting on emetic episodes, nausea assessment, and the amount of antiemetic therapy used. The authors of the study examined the observed incidence rates of acute and delayed CINV with the physician and nurse predictions. The surprising results demonstrated that physicians and nurses (while accurately predicting the incidence of acute CINV) underestimated the incidence of delayed CINV after HEC by 21% and 28%, respectively. The HCPs underestimated the incidence of delayed nausea after MEC by 28%; more than 75% of physicians and nurses underestimated the incidence of delayed CINV after HEC and MEC treatments.7
Comparable studies in other countries found similar results. In an Asian study of 107 patients and 37 medical providers (including 20 oncology nurses), medical providers were found to significantly overestimate the incidence of acute vomiting by 20% in HEC and MEC patients, respectively, but underestimated the incidence of delayed vomiting in MEC by 16%.8 For nausea, the providers were accurate in their estimation of acute and delayed nausea in HEC, but significantly underestimated the incidence of acute and delayed nausea (by 16% and 30%) in MEC patients.8 Healthcare providers in Mexico studied 82 patients receiving HEC and MEC and were found to significantly underestimate the incidence of delayed CINV after HEC (75.4% of the patients reported delayed nausea and the HCP predicted 41.7%; for delayed emesis, 63.2% of the patients reported having the symptom versus the HCP prediction of 31.8%).9
The aforementioned studies do not include the use of aprepitant, the NK-1 receptor antagonist approved in 2003. However, a study by Majem and colleagues10 did examine HCP perceptions versus patient reported incidence of CINV after the addition of aprepitant and found similar results. In a prospective observational study of patients receiving the first cycle of HEC regimens with platinum and without platinum or MEC was performed with 95 patients and 29 physicians and nurses. The HCPs overestimated the control of delayed CINV after both HEC and MEC, but were accurate in their prediction of the control of acute CINV. The authors concluded that both physicians and nurses overestimate the control of delayed CINV after HEC without platinum and after administration of MEC.10
It is clear that HCPs need to improve their awareness of the actual incidence of CINV; in particular the incidence of delayed CINV is often underestimated. The period of delayed CINV is difficult to assess as patients are often at home during this time period; without rigorous assessment or use of self-reporting tools such as a patient diary, this information may be not be captured. This underscores the importance of prescribing antiemetic regimens that cover both the acute period (when HCPs are often with the patient and can observe behavior) and the delayed period when patients are often at home. A recent study confirmed the fact that CINV continues to impact patients’ daily life, despite use of antiemetics; in particular the delayed period of symptoms were higher than the acute symptoms.11 In the current environment, we can reasonably assume that:
- Health care providers may underestimate the incidence and severity of CINV
- Appropriate use of combination antiemetic therapy is necessary to cover the acute and delayed period of CINV
- CINV continues to impact patient’s daily life despite recent improvements in therapy
Risk Factors for CINV
There are multiple risk factors for CINV; the patient and the chemotherapeutic regimen significantly contribute to the overall risk. Additional risk factors identified include younger patients (< age 50), those with a history of low alcohol consumption, gender (females are at higher risk), women with a history of morning sickness during pregnancy, and patients who experience motion sickness.5 Patients who had CINV with previous chemotherapy administrations are also at higher risk. Nursing assessment of patients scheduled to receive chemotherapy should include evaluation of the above risk factors; this evaluation will guide the HCP in the choice of the optimal antiemetic prophylaxis. Chemotherapy agents are stratified into four categories with regard to risk of emetogenicity.3

Based on information from Hawkins & Grunberg5; Multinational Association of Supportive Care in Cancer (MASCC)12; National Comprehensive Cancer Network (NCCN)13
Pathophysiology of CINV
A combination antiemetic approach is the most effective therapy for CINV; the existence of multiple emetic pathways requires agents with different activity to provide the most beneficial response.5 CINV occurs primarily via a peripheral and central pathway involving activation of neurotransmitters.14 Activation of the peripheral receptors occurs from local gastrointestinal irritation or damage. The central pathway is activated by the neurotransmitters in the chemoreceptor trigger zone (CTZ) by direct contact through blood or cerebrospinal fluid. Serotonin is primarily responsible for activation of the peripheral pathway; enterochromaffin cells (containing approximately 80% of the body’s serotonin) release this substance and induce emesis once bound to the serotonin receptors. The central pathway is the primary domain for substance P activation, which is present in the CTZ area of the brain (and in small amounts in the gastrointestinal tract).14 Additional receptors with activity in the vomiting response include the dopamine receptors, cannabinoids, histamine, acetylcholine and the muscarinic receptors: the GABAa and GABAß receptors may be involved as well, although these receptors are less defined with regard to their role in emesis.14
It is now accepted that the primary pathways implicated in CINV include the serotonin emetic pathway and the substance P pathway. Substance P, an 11-amino acid neuropeptide, binds to the NK-1 receptors and can induce emesis induced by opioids, ipecac, radiation and chemotherapy.15 A combination approach with the NK1 receptor antagonist, aprepitant, in conjunction with a serotonin antagonist and dexamethasone appears to provide significant protection against cisplatin-induced acute nausea and vomiting compared to serotonin antagonist and steroid alone; thus this approach is the currently accepted standard of antiemetic care for patients receiving HEC and for selected patients receiving MEC.13
Practice Guidelines
Clinical practice guidelines are important tools for HCPs; most guidelines incorporate evaluation of the currently available evidence to determine appropriate approaches to therapy. This evidence-based practice is critical to ensuring that patients receive the best care possible, supported by the best evidence.16 Guidelines often are driven by cost considerations as well, although focusing on just antiemetic costs can be problematic. Newer agents will almost always be more expensive than traditional therapies.17 The most relevant guidelines for the management of CINV include the Multinational Association of Supportive Care in Cancer (MASCC) guidelines, the National Comprehensive Cancer Network (NCCN), and the American Society of Clinical Oncology guidelines (ASCO).12,13,18 Most of the available guidelines stratify different agents according to the emetogenicity of the chemotherapy agent and contain recommendations for optimal antiemetic approaches. The ASCO guidelines have not been updated since 2006; however the NCCN and MASCC guidelines receive frequent updates as members of consensus panels strive to review and apply the most current data available.
NCCN, ASCO, and MASCC Guideline Recommendations
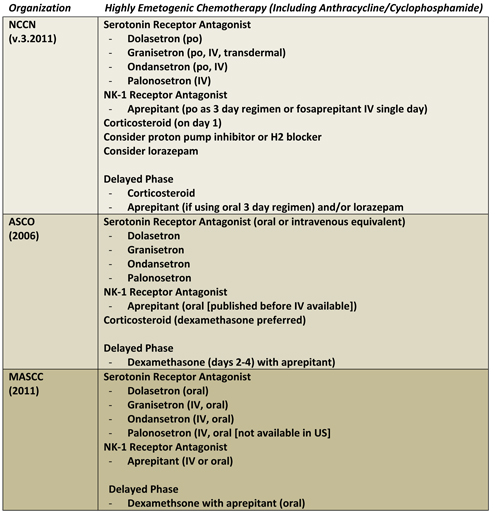
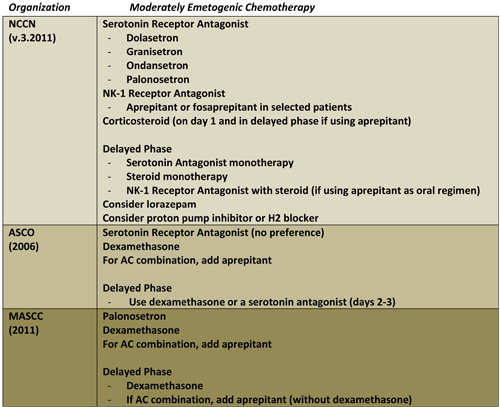
Based on information from MASCC, NCCN, and ASCO 12,13,18
Cost of Antiemetic Therapy
The costs of cancer treatment in the U.S. continue to rise. New therapies usually mean higher drug costs; the cost of aprepitant added to the previous standard of therapy increased costs, however even serotonin antagonists are not inexpensive. Uncontrolled CINV can produce costs not just for acquisition of agents but also related to the associated medical costs that can occur. These costs may include, but are not limited to: additional office visits or visits to the emergency room, costs associated with IV hydration, or even hospital admission. These factors can increase the overall costs of cancer care. With the approval of the novel NK-1 receptor antagonist, aprepitant, concerns over added costs were reported. Aprepitant is not a stand-alone agent and is most effective with the concomitant administration of a serotonin antagonist and corticosteroids, thus it is an added expenditure to the previous standard of therapy.
Selected Studies on Cost of Antiemetic Therapy
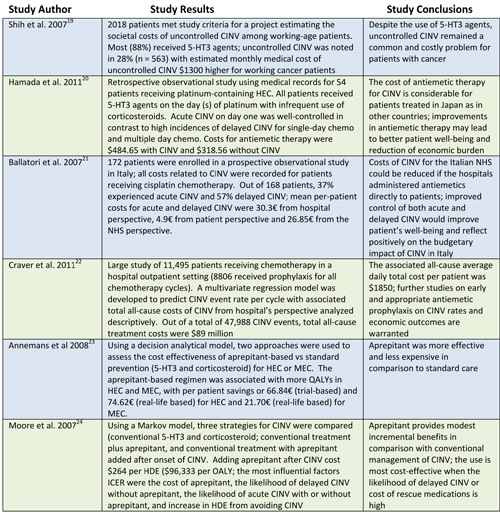
CINV (chemotherapy-induced nausea and vomiting); 5-HT3 (serotonin antagonist); HEC (highly emetogenic chemotherapy); MEC (moderately emetogenic chemotherapy); € (euro); QALYs (quality-adjusted life years); HDE (health day equivalent); ICER (incremental cost-effectiveness ratio)
However real the actual costs are when considering the cost of CINV, the ultimate cost of inadequate management of this symptom is to the patient who suffers one of the most dreaded side effects associated with therapy. Patients may consider cessation of potentially life-saving chemotherapy due to side effects such as CINV; the symptoms of nausea and vomiting are consistently ranked as significantly distressing to patients with cancer. Fear of continued or increasing CINV can lead anticipatory CINV which is inherently difficult to control. Inadequate initial management of CINV may also contribute to increased symptoms with later cycles of chemotherapy.
Advances in Antiemetic Approaches
Serotonin antagonists are available in oral and IV formulations. Although palonosetron is available in an oral formulation in Europe, only the IV form is currently available in the United States. It is important to note that the oral form of dolasetron is the only form currently recommended by the NCCN and MASCC guidelines. The NCCN guideline change reflects the most recent data on the IV formulation and the increased risk for QT, PR, and QRS prolongation and torsade de pointes.
- The United States Food and Drug Administration (FDA) announced on December 17, 2010 that the IV formulation of dolasetron should no longer be used for CINV in children or adults25
Granisetron was approved in a transdermal formulation in 2008 and offers patients an alternate delivery route for this antiemetic. Transdermal medication may be particularly useful for patients who cannot take or tolerate oral medications.26 The currently available product (Sancuso®) may be worn for up to seven days; it is important to remember that because transdermal medications often take 24 to 48 hours for full efficacy, patients must be educated to apply the patch a full day prior to anticipated chemotherapy treatment. Patients must also be educated to avoid excessive sweating or immersion in water as transdermal patches may peel off or loosen; hot, steamy environments can contribute to this as well.26 Side effects associated with the oral and intravenous (IV) serotonin antagonist class of agents also occur with transdermal granisetron, although in the clinical trials the incidence of constipation was approximately 7% (less than the commonly reported 10% in the literature for all serotonin antagonists) and headache occurred in less than 1% of patients.27
The approval of aprepitant in 2003 gave HCPs a new class of agent in the arsenal of drugs approved to treat CINV. The original trials were based on a regimen of three days of aprepitant, given in conjunction with a serotonin antagonist (ondansetron) and a corticosteroid compared to the standard of therapy at that time (serotonin antagonist with corticosteroid). Aprepitant approval was based on this data which showed a significant improvement in the management of CINV over the previous standard therapy of serotonin antagonist and corticosteroid (approximately 20% over the standard regimen).28 However, the three day regimen added to the cost of the antiemetics and adherence to the schedule could prove problematic for patients who encountered difficulty with reimbursement or filling of an oral prescription. The FDA approval of a single dose of IV fosaprepitant in a 115 mg dose in 2010 (which is being phased out) offered patients an intravenous option on day one, but the second and third day still required oral aprepitant.29
The recent approval of fosaprepitant as a single-dose 150 mg antiemetic therapy was based on data from the EASE study, a randomized, double-blind, active-control designed study of 2322 patients (2247 evaluable).4 Patients receiving HEC (cisplatin > 70 mg/m2) were randomly assigned to either a standard aprepitant regimen (125 mg on day one orally, followed by 80 mg orally on days 2 and 3) versus a single-dose fosaprepitant (150 mg on day 1). Both patient groups received ondansetron and dexamethasone with aprepitant or fosaprepitant. The primary end point was complete response (CR) [no vomiting or use of rescue medication]; secondary end points were CR during the delayed phase and no vomiting during the overall phase. Both regimens were equivalent within predefined bounds for noninferiority and both treatments were well-tolerated. The NK-1 receptor antagonists are considered standard of care for patients at high risk for CINV and the newly approved single day dose offers patients another therapeutic alternative to the previous three day regimen.4 Of note, HCPs should adjust the amount of corticosteroid in accordance with the regimen of aprepitant chosen.

Based on information from NCCN13
A second NK-1 receptor antagonist, casopitant, reached phase III clinical trials showing significant activity in the management of CINV in both HEC and MEC therapy. Although approval of this agent would have led to the availability of two NK-1 receptor antagonists for the treatment of CINV, the pharmaceutical company decided to withdraw their regulatory application for FDA approval after the FDA asked for additional safety data due to the anticipated higher costs of further study.30
Olanzapine, an atypical antipsychotic with activity in multiple neurotransmitters, has been studied in a number of phase II trials in combination with a serotonin antagonist and corticosteroid.13,14 The results of these trials have demonstrated a high rate of complete response and control of CINV. Although further studies are needed to completely evaluate the role of this novel therapy in CINV, the preliminary results are intriguing and worthy of further study. As a well-tolerated oral agent, this drug could be easily added to the current antiemetic approach commonly employed in the management of CINV.
Special Considerations: Corticosteroids
The clinical practice guidelines referenced in this paper all recommend the use of a corticosteroid, or more specifically the addition of dexamethasone, to the regimens used for management of both HEC and MEC. Methylprednisolone is an acceptable alternative agent and both drugs have been used safely and with success in the management of CINV.31 The exact mechanism of action for corticosteroids as an antiemetic is unknown, but data with methylprednisolone demonstrate that part of the therapeutic benefit is due to the agent’s ability to reduce serotonin release. Methylprednisolone has significant activity as prophylaxis against CINV in patients receiving various chemotherapeutic agents of all emetogenic levels.
Dexamethasone is also effective as monotherapy for the management of CINV. The optimal dose of corticosteroid in combination with serotonin receptor antagonists has not been definitively determined and the guidelines vary somewhat in their recommendations. Currently, the MASCC guidelines12 call for 20 mg PO of dexamethasone for HEC (12 mg PO when used with aprepitant or fosaprepitant), followed by 8 mg PO BID for 3-4 days (8 mg PO once daily when used with aprepitant or fosaprepitant). For moderate risk, 8 mg IV is recommended for the acute period, followed by 8 mg PO daily for 2-3 days. For low risk, the dose is 4-8 mg given once (without specifically recommending single or multiple day dosing).12
The NCCN guidelines13 for HEC recommend dexamethasone 12 mg PO or IV on day 1 with 8 mg po days 2-4, unless using aprepitant (see table for corticosteroid dosing above). For MEC, the dose is 12 mg po or IV, and if using steroid monotherapy in the delayed phase, the dose is dexamethasone 8 mg po or IV daily. Steroid use can produce gastrointestinal upset, therefore the NCCN recommendation to add a proton pump inhibitor or H2 blocker in an antiemetic regimen should be noted.13 Additionally, corticosteroids can increase blood sugar; extra monitoring may be considered in selected patients.
Nonpharmacologic Management of CINV
Dibble and colleagues32 presented interesting data on breast cancer patients receiving anthracycline-based chemotherapy who were randomized to receive acupressure or placebo. The researchers studied 160 women on their second or third cycle of therapy and randomized to receive acupressure to P6 point (active), acupressure to S13 point (placebo), or the usual care only. The subjects kept a daily log for 3 weeks. Although no significant differences were found in acute CINV or emesis in any of the treatment groups, the acupressure intervention in the delayed CINV group had a statistically significant reduction in the amount of vomiting and the intensity of nausea, compared with the placebo and usual-care groups.32 The researchers concluded that acupressure is safe and has efficacy in women with breast cancer who are on chemotherapy. Although this method should be studied further in other cancer types, it would be an inexpensive and easily implemented treatment strategy for CINV once initial training is completed.
Hypnosis and guided imagery have also been found to be helpful for some patients experiencing anticipatory CINV; selected botanicals may be of use as well. Caution should be exercised when using botanicals in patients with cancer; practitioners should have knowledge and experience in their use.33
Implications for Practice
Oncology nurses are well positioned to assess for and evaluate CINV in patients receiving chemotherapy. However, caution should be taken not to underestimate the percentage of patients suffering from this common side effect. Previous research has demonstrated that HCPs may not always be able to accurately assess the incidence and severity of CINV. Without proper assessment and questioning, this symptom may be underdiagnosed and therefore undertreated. Oncology nurses must be able to accurately determine the emetogenicity of chemotherapeutic regimens; clinical practice guidelines are available to guide the HCP in the appropriate antiemetic choice for specific regimens.
Communication of ineffective antiemetic coverage to appropriate members of the healthcare team is an essential role for the oncology nurse. The Oncology Nursing Society (ONS) Putting Evidence into Practice (PEP) 34 recommendations also have suggestions for oncology nurses in managing these patients and recommend smaller, more frequent meals, reduced food aromas, and milder foods to minimize symptoms of nausea, although evidence for those strategies is limited. Nonpharmacological approaches to the management of CINV may include the following:
- Self-hypnosis
- Relaxation and imagery
- Distraction
- Desensitization
- Acupressure
- Music therapy
- Biofeedback
Summary
Chemotherapy-induced nausea and vomiting remains a significant problem for patients; improvements in management of this side effect are needed. Although advances have been made, several critical issues remain of paramount importance. Health care providers, including oncology nurses, must be more accurate in their prediction of CINV risk for specific patients receiving chemotherapy. This assessment is essential to the initial choice of an appropriate antiemetic regimen for chemotherapy regimens. Increasing use of clinical practice guidelines can help HCPs determine optimal antiemetic therapy. Despite potentially higher acquisition costs for antiemetics, inadequately treated CINV can lead to increased resource costs for payers and institutions; however the most significant and ultimate cost is to the patient. This side effect remains one of the most distressing in cancer therapy; better control of this symptom can increase patient QoL and potentially improve adherence to therapy and patient outcome.
Assessment Tools and Clinical Practice Guidelines
Multinational Association of Supportive Care in Cancer (MASCC)
MASCC, an international multidisciplinary organization, is dedicated to research and education in all areas of supportive care, regardless of a patient’s stage of cancer. MASCC Guidelines were updated in 2011 and are available at: http://data.memberclicks.com/site/mascc/MASCC_Guidelines_English_2011.pdf Accessed May 9, 2011
National Cancer Institute (NCI) (US National Institutes of Health)
Classification and criteria for grading the severity of nausea and vomiting are useful assessment tools. Available at http://www.cancer.gov/cancertopics/pdq/supportivecare/nausea . Updated December 17, 2010 Accessed May 9, 2011.
Oncology Nursing Society (ONS)
The ONS has comprehensive information in their “Putting Evidence into Practice” (PEP) resources containing evidence-based interventions for nausea and vomiting. Available at: http://www.ons.org/Research/PEP/Nausea Accessed May 12, 2011.
American Society of Clinical Oncology (ASCO)
Nine oncology organizations participated in producing the ASCO Guideline for Antiemetics in Oncology: Update 2006. Go to: http://jco.ascopubs.org/content/24/18/2932.full.pdf Accessed May 9, 2011.
National Comprehensive Cancer Network (NCCN)
The NCCN promotes awareness of the importance of continuous improvement in quality of care and recognizes the significance of creating clinical practice guidelines appropriate for use by patients, clinicians, and other health care decision makers. The home page at http://www.nccn.org/ offers links to guidelines for patients and professionals; click on Clinical Practice Guidelines in Oncology. The full NCCN Clinical Practice Guideline for Antiemesis can be reached after free registration on the site. Available at http://www.nccn.org/professionals/physician_gls/pdf/antiemesis.pdf Accessed May 9, 2011.
References
- Roila, F, Herrstedt, J, Gralla, RJ et al. Prevention of chemotherapy-and radiotherapy-induced nausea and vomiting: Guideline update and results of the Perugia consensus conference. Support Care Cancer 2011; 19 [Suppl 1]: S63-S65. doi:10.1007/s00520-010-1044-1
- Cohen, L, de Moor, CA, Eisenberg, P et al. Chemotherapy-induced nausea and vomiting: incidence and impact on patient quality of life at community oncology settings. Support Care Cancer 2007; 15 (5): 497-503. doi:10.1007/s00520-006-0173-z
- Jordan, K, Sippel, C, Schmoll, HJ. Guidelines for antiemetic treatment of chemotherapy-induced nausea and vomiting: Past, present, and future recommendations. Oncologist 2007; 12: 1143-1150. doi:10.1634/theoncologist.12-9-1143
- Grunberg, S, Chua, D, Maru, A et al. Single-dose fosaprepitant for the prevention of chemotherapy-induced nausea and vomiting associated with cisplatin therapy: randomized, double-blind study protocol – EASE. J Clin Oncol 2011; 29: 1495-1501. doi:10.1200/JCO.2010.31.7859
- Hawkins, R & Grunberg, S. Chemotherapy-induced nausea and vomiting: Challenges and opportunities for improved patient outcomes. Clin J Oncol Nurs 2009; 13 (1): 54-64. doi:10.1188/09.CJON.54-64
- Bloechl-Daum, B, Deuson, RR, Mavros, P et al. Delayed nausea and vomiting continue to reduce patients’ quality of life after highly and moderately emetogenic chemotherapy despite antiemetic treatment. J Clin Oncol 2006; 24:4472:78. doi:10.1200/JCO.2006.05.6382
- Grunberg, SM, Deuson, RR, Mavros, P et al. Incidence of chemotherapy-induced nausea and emesis after modern antiemetics: Perception versus reality. Cancer 2004; 100:2261-2268. doi:10.1002/cncr.20230
- Liau, CT, Chu, NM, Liu, HE et al. Incidence of chemotherapy-induced nausea and vomiting in Taiwan: Physican’s and nurses estimation vs. patients’ reported outcomes. Support Care Cancer 2005; 13 (5): 277-86. doi:10.1007/s00520-005-0788-5
- Erazo, VA, Wisniewski, T, Figueroa, VJI, et al. Incidence of chemotherapy-induced nausea and vomiting in Mexico: Health care provider predictions versus observed. Curr Med Res Opin 2006; 22 (12): 2403-10. doi:10.1185/030079906X154033
- Majem, M, Moreno, ME, Calvo, N et al. Perception of healthcare providers versus patient reported incidence of chemotherapy-induced nausea and vomiting after the addition of NK-1 receptor antagonists. Support Care Cancer 2010; Nov 18. [epub ahead of print]. doi:10.1007/s00520-010-1042
- Hilarius, DL, Kloeg, PH, van der Wall, E et al. Chemotherapy-induced nausea and vomiting in daily clinical practice: a community hospital-based study. Support Care Cancer 2011, doi:10.1007/s00520-101-1073-9
- Multinational Association of Supportive Care in Cancer (MASCC). MASCC/ESMO Antiemetic Guideline 2011. Retrieved from: http://data.memberclicks.com/site/mascc/MASCC_Guidelines_English_2011.pdf
- National Comprehensive Cancer Network (NCCN). NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines™) Antiemesis v 3.1011. Retrieved from: http://www.nccn.org/professionals/physician_gls/pdf/antiemesis.pdf (Free registration required.)
- Frame, DG. Best practice management of CINV in oncology patients: I. Physiology and treatment of CINV. J Support Oncol 2010; 8 (2 Suppl 1): 5-9
- Roila, F, Fatigoni, S, & Ciccarese, G. Daily challenges in oncology practice. What do we need to know about antiemetics? Ann Oncol 2006; 17 (Suppl 10): x90-x94. doi:10.1093/annonc/mdl1244
- Moore, S. Evidence-based practice. In press; www.managecrc.com
- Wickham, R. Best practice management of CINV in oncology patents: II. Antiemetic guidelines and rationale for use. J Support Oncol 2010; 8 (suppl 1):10-15.
- Kris, M, Hesketh, PJ, Somerfield, MR et al. American Society of Clinical Oncology Guideline for Antiemetics in Oncology: Update 2006. J Clin Oncol 2006; 24: 2932-2947. doi:10.1200/JCO.2006.06.9591 Retrieved from: http://jco.ascopubs.org/content/24/18/2932.full.pdf
- Shih, TYC, Xu, Y & Elting LS. Costs of uncontrolled chemotherapy-induced nausea and vomiting among working-age cancer patients receiving highly or moderately emetogenic chemotherapy. Cancer, 2007; 110 (3): 678-85. doi:10.1002/cncr.22823
- Hamada, S, Hinotsu, S, Hori, K et al. The cost of antiemetic therapy for chemotherapy-induced nausea and vomiting in patients receiving platinum-containing regimens in daily practice in Japan: a retrospective study. Support Care Cancer 2011; [epub ahead of print]. doi:10.1007/s00520-011-1155-3
- Ballatori, E, Roila, F, Ruggeri, B et al. The cost of chemotherapy-induced nausea and vomiting in Italy. Support Care Cancer 2007; 15 (1): 31-8. doi:10.1007/s00520-006-0094-x
- Craver, C, Gayle, J, Balu, S et al. Clinical and economic burden of chemotherapy-induced nausea and vomiting among patients with cancer in a hospital outpatient setting in the United States. J Med Econ 2011; 14: 87-98. doi:10.3111/13696998.2010.547237
- Annemans, L, Strens, D, Lox, E et al. Cost-effectiveness analysis of aprepitant in the prevention of chemotherapy-induced nausea and vomiting in Belgium. Support Care Cancer, 2008; 16 (8): 905-15. doi:10.1007/s00520-007-0349-1
- Moore, S, Tumeh, J, Wojtanowski, S et al. Cost-effectiveness of aprepitant for the prevention of chemotherapy-induced nausea and vomiting associated with highly emetogenic chemotherapy. Value Health 2007; 10 (1): 23-31.
- United States Food and Drug Administration (FDA). FDA Drug Safety Communication: Abnormal heart rhythms associated with the use of Anzemet (dolasetron mesylate). Retrieved from: http://www.fda.gov/drugs/drugsafety/ucm237081.htm
- Schulmeister, L. Granisetron transdermal system: A new option to help prevent chemotherapy-induced nausea and vomiting. Clin J Oncol Nurs 2009; 13 (6): 711-714. doi:10.1188/09.CJON.711-714
- Tuca, A. Use of granisetron transdermal system in the prevention of chemotherapy-induced nausea and vomiting: a review. Cancer Manag Res 2009; 2: 1-12. doi: 10.2147/CMR.S4953
- Campos, D, Pereira, JR, Reinhardt, RR et al. Prevention of cisplatin-induced emesis by the oral neurokinin-1 antagoinist, MK-869, in combination with granisetron and dexamethasone or with dexamethasone alone. J Clin Oncol 2001; 19: 1759-67.
- Hesketh, PJ. Prevention and treatment of chemotherapy-induced nausea and vomiting. UpToDate. Retrieved from: http://www.uptodate.com/contents/prevention-and-treatment-of-chemotherapy-induced-nausea-and-vomiting Accessed May 23, 2011.
- Feyer, P & Jordan, K. Update and new trends in antiemetic therapy: the continuing need for novel therapies. Ann Oncol 2011; 22: 30:38. doi:10.1093/annonc/mdq600
- Grunberg, SM. Antiemetic activity of corticosteroids in patients receiving cancer chemotherapy: dosing, efficacy, and tolerability analysis. Ann Oncol 2006; 18: 233-240. doi:10.1093/annonc/mdl347
- Dibble S. Acupressure for chemotherapy-induced nausea and vomiting: a randomized clinical trial. Oncol Nurs Forum. 2008; 34:813-820.
- Mansky, PJ & Wallerstedt, DB. Complementary medicine in palliative care and cancer symptom management. Cancer J 2006; 12 (5): 425-31.
- Oncology Nursing Society. Putting evidence into practice recommendations for chemotherapy induced nausea and vomiting. Retrieved from http://www.ons.org/Research/PEP/Nausea Accessed May 12, 2011.
|